Use Glutamine To Reduce The Severity Of Mucositis And Neuropathy (During Chemotherapy Or Radiation Therapy)
If you are about to start a course of chemotherapy that can cause mucositis (i.e. of the mouth, throat or esophagus) or peripheral neuropathy (i.e. hands and feet), ask your oncologist if you can use glutamine to help reduce the severity of these common symptoms.
If you are going to receive radiation therapy to the head, neck or chest (specifically, anywhere near the esophagus), Glutamine can be helpful to reduce the development of severe mucositis in these tissues.
**Did you know that honey is also a proven therapy for mucositis? Read my previous blog entry on honey and mucositis.**
HERE ARE THREE COMMONLY USED REGIMENS IN THE PREVENTION OF MUCOSITIS (ORAL, THROAT OR ESOPHAGEAL) AND PERIPHERAL NEUROPATHY:
You can buy glutamine (usually in the form of L-glutamine), in powder, capsule, tablet, or liquid form. However, I recommend using the powder form of L-glutamine, and mixing it in with cold or room temperature liquids (water or juice.) It should not be added to hot beverages because heat destroys glutamine. Glutamine therapy works best if started at the time of beginning radiation therapy or chemotherapy. It will be less effective if you start this after already showing signs or symptoms of mucositis or peripheral neuropathy.
For the prevention of oral mucositis (OM)
Mix 10 grams of powdered glutamine in a small glass (6-8 ounces) of water or juice. Swish and gargle for 30-60 seconds and swallow. You can continue to do this until the 6-8 ounces are gone. Repeat every 8 hours (schedule: morning, mid-day, evening)
Start this regimen on the first day of chemotherapy and continue for 14 days after the last dose of chemotherapy in patients who do not develop OM or until 5 days after resolution of OM for patients who experienced OM.
Other recommendations:
Refrain from eating or drinking for 30 minutes after dosing.
Adhere to good oral hygiene practices and gently brushed their teeth twice daily, 30 minutes or more after using glutamine, using a soft toothbrush and fluoride toothpaste.
Daily flossing and an alcohol-free fluoride rinse is recommended.
This is based on a study that showed a significant reduction in OM among patients using oral glutamine.
These investigators used a proprietary glutamine suspension (Saforis, MGI Pharma, Inc., Bloomington, MN), which was administered at a dose of 2.5 g per 5 mL 3 times per day for a total daily dose of 7.5 g. This product reportedly is able to be better absorbed into the oral mucosa than standard glutamine. (I believe that this can be compensated for by using a higher dose, 10 grams, 3-times per day, of standard glutamine, as recommended above.)
Various chemotherapy regimens used in this study (21-day cycle): cyclophosphamide, doxorubicin, and 5-fluorouracil (CAF); 5-fluorouracil, doxorubicin, and cyclophosphamide (FAC); or doxorubicin and cyclophosphamide (AC).
Compared with placebo, glutamine significantly reduced the incidence of moderate-to-severe OM 39% vs. 50% (placebo.)
For prevention of mucositis of the throat and esophagus (esophagitis) from radiation and chemotherapy:
Mix 10 grams of powdered glutamine in a small glass (6-8 ounces) of water or juice. Drink (swallow). Repeat every 8 hours (schedule: morning, mid-day, evening)
Start this regimen 1 week before radiation therapy and continue for 2 weeks after completion of radiation therapy.
This is based on a study that showed a significant reduction in esophagitis among patients receiving this regimen versus no glutamine:
There was minimal-to-no-esophagitis was seen in 71% of the glutamine supplemented patients versus only 44% without glutamine
By the end of treatment, the glutamine supplemented patients gained 2.6 kg (median), while those without glutamine lost 3.3 kg (median)
There was a significant delay to the time of first noticing esophagitis in the glutamine patients versus the non-glutamine patients: 25 days versus 16 days.
There were also fewer treatment breaks, hospitalizations and late esophageal toxicities among the patients who took glutamine versus those who did not.
Importantly, there were no differences in cancer recurrence rates at 24 months of follow-up (the glutamine did not reduce the effectiveness of treatment.)
For the prevention of chemotherapy-induced peripheral neuropathy (studied with oxaliplatin and paclitaxel)
Mix 15 grams of powdered glutamine in a small glass (6-8 ounces) of water or juice. Drink. Repeat every 12 hours (schedule: morning and evening)
Start this regimen on the day of oxaliplatin infusion and continue for seven days thereafter. Repeat with each infusion.
This is based on a study that showed a significant reduction in chemotherapy-induced peripheral neuropathy among patients receiving this regimen versus no glutamine:
After all 6 cycles of chemotherapy, 48% of patients in the glutamine group had no peripheral neuropathy (PN) versus only 27% in the non-glutamine group.
After all 6 cycles of chemotherapy, 12% of the patients in the glutamine group had moderate-to-severe PN versus 32% in the non-glutamine group.
Glutamine supplementation significantly improved cold intolerance and lessened the interference to activities of daily living.
Chemotherapy dose-reductions were less frequently needed in the glutamine patients (7%) versus those not taking glutamine (27%)
There were no differences found in the response to chemotherapy or survival between the two groups.
HOW DOES GLUTAMINE REDUCE MUCOSITIS AND ESOPHAGITIS?
Glutamine has been shown to reduce the degree of mucositis through:
anti-inflammatory mechanisms (inhibition of one of the main switches that turn on inflammation, NF-kappaB)
inhibition of bacterial toxins
increased tissue healing (increased fibroblast and collagen synthesis.)
HOW DOES GLUTAMINE REDUCE CHEMOTHERAPY-INDUCED PERIPHERAL NEUROPATHY?
We don’t know exactly, however it is believed that glutamine may exert its neuroprotective effects by upregulation of nerve growth factor. In animal studies, supplementation with glutamine appears to increase NGF.
IS GLUTAMINE SAFE TO GIVE TO PATIENTS WITH CANCER?
This is an area of controversy, as it is well-known that under certain circumstances cancer cells use glutamine for energy even more voraciously than glucose.
However, no human study, have ever shown that glutamine increased tumor growth rates or decreased the efficacy of other cancer therapies.
Over the last 20 years, 36 clinical studies have demonstrated the tolerance, safety and effects of glutamine (oral and IV) in patients undergoing chemotherapy and/or radiation therapy. In each of these studies, researchers have reported that glutamine supplementation in cancer patients improves their metabolism and clinical situation without increasing tumor growth.
Potential Side Effects and Drug Interactions:
Generally, very well-tolerated and is considered safe for use by most people for the duration of cancer care (chemotherapy and/or radiation therapy) in doses up to 40 grams per day (adults.)
Do not use glutamine if you:
Have kidney failure, kidney dysfunction, or if your kidney function is impaired or abnormal.
Have liver failure, liver dysfunction, or if your liver function is impaired or abnormal.
Have ever been diagnosed with or had a period of hepatic encephalopathy (liver function that affects your mental, emotional, or cognitive state).
Have a history of mental illness, especially bipolar depression (manic depression), mania, or hypomania.
Have a history of seizure disorders, such as epilepsy or are taking medications to control a seizure disorder.
Have a history of allergic reaction to monosodium glutamate (MSG), a flavoring agent sometimes used in the preparation of Chinese food in restaurants.
Are taking or have been prescribed to take a medication called lactulose.
Adverse drug-glutamine interactions are not common, but (as with any supplement) always check with your physician before starting glutamine.
|
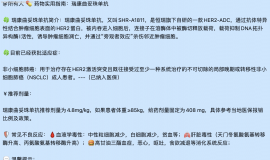
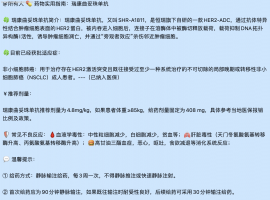 汇总4月最新:临床试验招募| 小细胞
"化疗±免疫后进展了,还能怎么办?"——这是许多小细胞肺癌患者和家属的困境。
临
汇总4月最新:临床试验招募| 小细胞
"化疗±免疫后进展了,还能怎么办?"——这是许多小细胞肺癌患者和家属的困境。
临
 新人求助
我爸爸身体不适 26 年 4 月 10 号去医院检查,初步结果是肺肿可能是肺癌,因年纪大 7
新人求助
我爸爸身体不适 26 年 4 月 10 号去医院检查,初步结果是肺肿可能是肺癌,因年纪大 7
 母亲肺腺癌晚期骨转移,EGFR21突变,
母亲1970年出生,56周岁,身高163cm,体重98kg(196斤)。2025年9月23日肺炎住院,胸
母亲肺腺癌晚期骨转移,EGFR21突变,
母亲1970年出生,56周岁,身高163cm,体重98kg(196斤)。2025年9月23日肺炎住院,胸
 肺癌术后五年,脑膜转移治疗三年,伏
2025年8月14日更新: 终于输液港血培养结果为阴性了,14天美平消炎出院了,昨天开始双
肺癌术后五年,脑膜转移治疗三年,伏
2025年8月14日更新: 终于输液港血培养结果为阴性了,14天美平消炎出院了,昨天开始双
 从6个月到1400多天:一位晚期肺癌患
2026年全国肿瘤防治宣传周(4月15日-21日)即将到来,今年中国抗癌协会的主题是“肿瘤
从6个月到1400多天:一位晚期肺癌患
2026年全国肿瘤防治宣传周(4月15日-21日)即将到来,今年中国抗癌协会的主题是“肿瘤







 显身卡
显身卡