非小细胞肺癌中的PTEN突变及其与EGFR、ERBB2、KRAS和TP53突变的关系
7 B8 L) h, j8 ?- V9 B& l" R, I) ~PTEN mutations and relationship to EGFR, ERBB2, KRAS, and TP53 mutations in non-small cell lung cancers
% M7 P7 M" l# F1 @7 q- z作者:Jin G, Kim MJ, Jeon H-S, Choi JE, Kim DS, Lee EB,
' k- [7 B* f: M. Y" D# e期刊: 《LUNG CANCER》2010年9月3期69卷 / m# i0 N2 E$ t8 C! |( G( s, Z( g
+ O4 T6 r# k) [& m ~! J; ]4 ]
Somatic mutations of phosphatase and tensin homolog deleted on chromosome ten (PTEN) in non-small cell lung cancers (NSCLCs) have been investigated in but a small number of cases. In addition, the relationship between PTEN mutations and epidermal growth factor receptor (EGFR), KRAS, and TP53 mutations has not been investigated. Therefore, we investigated the frequency of PTEN mutations in 176 surgically resected NSCLCs and analyzed the relationship between PTEN mutations and EGFR, ERBB2, KRAS, and TP53 mutations. Mutations of PTEN (exons 1-9), EGFR (exons 18-21), ERBB2 (exons 19 and 20), KRAS (exon 1), and TP53 (exons 2-11) were determined by polymerase chain reaction and direct sequencing. PTEN mutations were present in 8 (4.5%) of the 176 tumors. PTEN mutations were only found in ever-smokers and were significantly more frequent in squamous cell carcinoma than in adenocarcinoma (10.2% vs 1.7%, P= 0.02). Mutations of EGFR, ERBB2, KRAS, and TP53 genes were found in 36 (20.5%), 2 (1.1%), 11 (6.3%), and 66 (37.5%) cases, respectively. Of the 8 tumors with PTEN mutations, 1 case concurrently had an EGFR mutation and 4 cases had TP53 mutations. However, PTEN mutations were not found in the tumors with KRAS mutation. Our findings indicate that PTEN mutations are relatively common in NSCLC, and thus analysis of PTEN mutations may facilitate a comprehensive understanding of the genetic alterations related to the EGFR signaling pathway.
+ e8 d6 J, l; e: R |
 ROS1肺癌重磅靶向药开出首方,此类患
作者:雨过天晴
“瑞普进了”,在新版医保目录发布后,一位患者家属在微信群内激动地
ROS1肺癌重磅靶向药开出首方,此类患
作者:雨过天晴
“瑞普进了”,在新版医保目录发布后,一位患者家属在微信群内激动地
 肺腺癌3a期术后应该化疗加靶向还是单
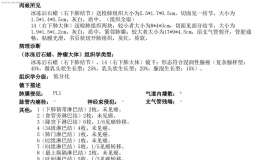
术前CT显示无任何淋巴结肿大,但原发灶有胸膜牵拉,血管集束,且有多发小结节(外科认
肺腺癌3a期术后应该化疗加靶向还是单
术前CT显示无任何淋巴结肿大,但原发灶有胸膜牵拉,血管集束,且有多发小结节(外科认
 EGFR靶向治疗常见耐药机制,治疗药物
作者:Tony
大约在40年前,间质-上皮细胞转化因子(MET)基因被发现,其位于7号染色体
EGFR靶向治疗常见耐药机制,治疗药物
作者:Tony
大约在40年前,间质-上皮细胞转化因子(MET)基因被发现,其位于7号染色体
 肺鳞癌术后中期寻求后续治疗方案
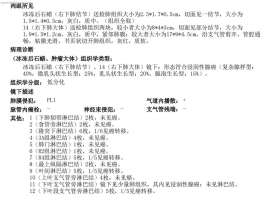
无术前辅助治疗,术后病理高危因素较多。病人无其他基础疾病,实际年龄47,身体素质较
肺鳞癌术后中期寻求后续治疗方案
无术前辅助治疗,术后病理高危因素较多。病人无其他基础疾病,实际年龄47,身体素质较
 口服紫杉醇来了,告别繁琐治疗,你准
作者:王川
想象一下,化疗不再需要频繁去医院,不再需要忍受长时间的静脉注射。你可
口服紫杉醇来了,告别繁琐治疗,你准
作者:王川
想象一下,化疗不再需要频繁去医院,不再需要忍受长时间的静脉注射。你可






 显身卡
显身卡